JOSR Journal of Pharmacy and Biological Sciences (IOSR-JPBS) e-ISSN:2278-3008, p-ISSN:2319-7676. Volume 11, Issue 5 Ver. II (Sep. -Oct.2016), PP 38-41www.iosrjournals.orgDOI: 10.9790/3008-1105023841www.iosrjournals.org 38| Page
![]()
The revival of an ancestral galenic preparation called “Ceratum” apt to re-establish thenormal viscoelasticity of dermisin perilous skin diseases like iatrogenic dyshidrosis andto treat scars after milia removal.
Texia Research ¹, Lorenzo Martini²
¹Texia Research-Eu-TURIN, ² Department of Pharmaceutical Biotechnologies University of Siena
Abstract: Scope of our research is to paving the way for a revival of a very old galenicpreparation, that is nort oily or waxy, and so it cannot be baptized as ointment or unguentum.But the Trojan horse is that medical device I ideated (and its modus operandi is quite difficult and artful) is capable to re-establish an optimal viscoelasticity to dermal component of human skin and moisture at niveau of the stratum corneum in pathological cases that are rare and commonly impossible to be treated, as iatrogenic dyshidrosis and the suppurative state of skin when eruptive milia are removed physically from skin in order to obtain a restitutio ad integrum that is perfect and absolutely free from anomalies.
Keywords: Ceratum, iatrogenic dyshidrosis, eruptive milia, Rombo syndrome, ballistometer
I.Background
Ceratumis an ancient term to indicate a sort of ointment capable to strongly adhere to epidermis and create a viscous but resistant film upon the stratum corneum slowly and progressively, permitting to all the ingredients that are inserted in formula to penetrate deeply and regularly through the skin at all. For example an old U.S.P. refers about the Ceratum Juniperi Virginiani and the Ceratum Resinosus, a supplement of a British Pharmacopoeia by Samuel Frederick Gray, 1821, records the Ceratum citrinum and the Ceratum cerae et resinae flavae,in the Pharmacopoeia Collegii Regalis Medicorum Londinensis (1824), the Ceratum Sabinae, the Ceratum saponis, the Ceratum resinae (yclept Yellow Basilicon), the Ceratum Plumbi compositum, the Ceratum Plumbi acetati, the Ceratum calaminae yclept Epulotic Cerate and the Cerate of Spanish fly.The Mexican Pharmacopoeia of 1885 refers about the Ceratum cosmeticum anglicum e centuries of other cerates that are to be recorded in the Annals of History. All cerates were prepared melting yellow wax and stirring slowly cold olive oil and all the other ingredients to obtain the appropriate Ceratum.I have created a modern ceratum, based on the same ancestral method of proceeding, using white wax, because present a lower melting point and jojoba wax, besides squalane,ceramides and shea butter.The innovation of this revisited ceratum is the Jojoba oil, that is considered as chief ingredient and not an emollient: jojoba oil contains the 76% of 11-eicosanoic acid, a monoinsaturad fatty acid (20 C) that is responsible of creating the flexible and strong barrier upon the stratum corneum, so that the aqueous vapour cannot poor out absolutely.By this way, even if the patient spreads the Ceratum in a cold and dry day, all the wetness inside his dermis remains at intracellular niveau, and if he spreads it during a wet and hot day, the lypophilic layer impedes the pooring out of all hydrosoluble elements from inside. Ceratum is dedicated most of all to all types of iatrogenic skin disydrosis and is suggested after the removal of eruptive milia expecially in childhood, in order to avoid they could become cysts and/orremain as connotation signalson face for all life.Iatrogenic skin dyshidrosis is often evoked by long term therapies that are used to combat several malaises or by physical methods for diagnose other diseases or cure or after surgical operations, and so, for instance, among the dyshidrosis caused by prolonged use and abuse of medicaments, manifolds medications against Folate deficiency, thalaxemia, Hyperglycemia, Nelson syndrome/ACTH secreting,(1)lichen planus, dermatitis herpetiformis, erythema multiforme, pompholyx, autoimmune progesterone dyshidrosis, induced pemphigus/penicillamine xerosys, Dumping Syndrome,(2) Chronic dysentery, Bacterial folliculitis,Fibrositisand finally abuse of antidepressants; among the physical methods of diagnose the Radiation/ionizing/xray and among the post surgical operations the bilateral adrenalectomy and sometimes after some types of traumatic situations. Milia, on the other hand, are benign, keratinous cysts that commonly manifest as tiny white bumps on the face of the newborn. When present on the gum margin, they are referred to as Bohn’spots. Milia can be broadly categorized into primary and secondary types. Congenital milia in newborns account for the vast majority of primary milia. Primary milia may also occur in association with one of several genodermatoses or sporadically without associated findings. Secondary milia may be associated with an underlying skin disease, medications, or trauma.Berk and Bayliss published an updated classification of milia, as follows (3)Primary miliamay be:Congenital, Benign primary milia of children and adults, Milia en plaque ,Nodular grouped milia, Multiple eruptive milia ,Nevus depigmentosus with milia, genodermatosis.Secondary milia are often associated to abuse of medications or post-traumatic conditions.Benign acquired milia of children and adults also occur spontaneously; however, like other acquired milia, they have a tendency to persist without treatment. Benign acquired milia of children and adults favor the eyelids, cheeks, forehead andgenitalia.Multiple eruptive milia describes acquired and widespread milia that appear rather abruptly over weeks to months. Multiple eruptive milia may be associated with a genodermatosis or inherited in an autosomal dominant fashion without other apparent anomalies; however, in most cases they occur sporadically.Genodermatosis-associated milia have been reported in association with basal cell nevus syndrome, (4) Rombo syndrome, (5) Brooke-Spiegler syndrome, (6) pachyonychia congenita type 2, (7)and atrichia with papular lesions.(8)In children, traumatic milia most commonly manifest following abrasions or burns. Milia have also been reported following skin grafting. Milia may occur in association with blistering skin diseases. Epidermolysis bullosa and porphyria cutanea tarda are the classic examples. Milia associated with topical corticosteroid use is rarely reported. (9)The most common type of milia removal is performed using a needle. Once the skin with milia has been cleaned, a sterile needle is then used to create an tiny incision in the skin covering the cyst and the contents of the milia are carefully extracted so as not to cause any trauma to theskin.Certain types of milia may not be suitable for this type of removal, and may need to be treated using a hyfrecator. A hyfrecator works to cauterize the skin covering the milia by using tiny electrical pulses then allowing the contents to be extracted.In other cases it may be more suitable to be prescribed a topical medication to treat the milia, but this is only for certain types of milia, especially the eruptive ones and nodular grouped milia.(10-11)The best treatment will depend upon the type of milia as well as the location and number of milia that need to be removed.Beauticians suggest treatments by using a non-abrasive exfoliating cleanser and vitamin A product on a regular basis. Milia tend generally to recur, after gentle microabrasion. These products will soften the skin that covers the milia, making it easier to remove and can also help prevent further milia developing.After the removing of milia, the upper three layers of epidermis are injured, and the risk of a misleading cicatrisation (almost at the very first step, the inflammatory one, when tissues may undergo bacterial assaults) is to be exorcised.For this, I created a Ceratum, apt to create a sort of thick waxy film, that owing to its lypophily tends to suffocate all bacteria Gram positive and Gram negative.
II.Materials and methods
We have recruited 4 (four) volunteers who willingly made up their mind to undergo our experimentations for nine (9) days and we have used a ballistometer (Dia-Strom torsional ballistometer) to evaluate the increase of the hydration and degree of viscoelasticity of their skin and derma.The individuals were:1) one middle age woman suffering from Saurat-Kaya’s syndrome.the clinical manifestations of the syndrome that is designed even as dermatoporosis comprise morphological markers of fragility–rather trivial–such as senile purpura, stellate pseudoscars and skin atrophy, and functional expression of skin fragility resulting from minor traumas such as frequent skin laceration, delayed wound healing, nonhealing atrophic ulcers and subcutaneous bleeding with the formation of dissecting hematomas leading to large zones of necrosis. She can never stay at the sun rays, even in winter and has to use always total block screen emulsions, and the most important manifestation of the syndrome is under her eyes and onto cheekbones. 2) oneold woman (75 y.old) presenting so dry and chapped lips that no lipstick or rouge can adhere onto the buccal mucosa.3) one child with milia under eyes and eyelids(the measures by ballistometer were carried out only after the third day of application of Ceratum) 4) one middle age woman suffering from the Rombo’s syndrome.It s a very rare genetic disorder characterized mainly by atrophoderma vermiculatumof the face, multiple milia, telangiectases, acral erythema peripheral vasodilation with cyanosis(12)and a propensity to develop basal cell carcinomas(13)The lesions become visible in late childhood, began at ages 7 to 10 years and are most pronounced on the face,At that time a pronounced, somewhat cyanotic redness of the lips and hands was evident as well as moderate follicular atrophy of the skin on the cheeks. In adulthood, whitish-yellow, milia-like papules and telangiectatic vessels developed. The papules were present particularly on the cheeksaand forehead, gradually becoming very conspicuous and dominating the clinical picture. Trichoepitheliomas were found in 1 case. In adults, the eyelashes and eyebrows were either missing or irregularly distributed with defective and maldirected growth. Basal cell carcinomas were a frequent complication. The skin atrophy was referred to as vermiculata atrophoderma. Basal cell carcinomas may develop around the age of 35. Histological observations during the early stage include irregularly distributed and atrophic hair follicles, milia, dilated dermal vessels, lack of elastin or elastin in clumps. As in the precedent case the measures using the ballistometer were performed only afyter the third day of application of the Ceratum.The Ballistometer is an instrument designed to evaluate in vivo, in a non-invasive manner, the viscoelastic properties of the skin by analyzing the bounce pattern of a pendulum-like probe as it impacts on the skin. The kinetic energy of the probe striking the skin is stored by the elastic components of the skin and is then released, causing the probe to rebound. Since the skin is a viscoelastic, anisotropic material, the height of the probe rebound is influenced by the amount of stored energy lost in the viscosity of the skin. In this manner, the Ballistometer measures the capacity of the skin to absorb mechanical energy, and it assesses mostly the behavior of the tissues underlying the stratum corneum.Results are graphically represented by a curve where several factors are responsible of the final values (recorded as coefficient of restitution) that range from 0 to 1 mm.The aforesaid factorscorrespond to α) Indentation: the peak penetration depth of the probe tipbeneath the skin level (skin datum))K: the start height of the probe tip above the skinsurface. This is directly related to the energy stored inthe torsion wireγAlpha: the rate of energy damping. Large values indicateenergy absorbent (in-elastic) samplesδ) Coefficient of Restitution –CoR: a high value indicates ahighly elastic sampleε) Area: the area between the bounce profile and the skinzero datumThecurve is represented like the following, where it is possible to observe that the real values go from 0 and 1mm.Here follows a graphical example of a curve obtained by using a torsional ballistometer.
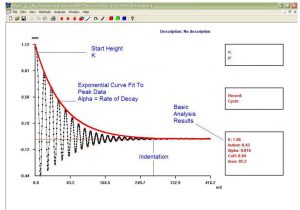
These values are derived form the heights of the first and second rebounds, measured as the amplitude of the angular displacement of the probe. The heights of thefirst and second rebounds correlate directly with the elasticity of the skin, in that a more elastic material yields a higher bounce when struck by the probe than a less elastic material, assuming equivalent viscosity (Fthenakis, et al. 1991). While thesevariables are commonly considered indicators of the elastic nature of the skin, the amplitude and/or number of displacements of the probe can convey other qualities, such as the firmness or softness of the skin (Jemec et al. 2001). The coefficient of restitution relates to the proportion of the maximum height that the probe rebounds after striking the skin. The coefficient of restitution can range from 0, if the impact was completely devoid of elasticity, to 1, which is a theoretical state of complete elasticity (Fthenakis, et al. 1991).In Table I one can notice that the values recorded after measure by wire torsion using the ballistometer tend all to increase (Case 3 and 4, obviously, as aforesaid, only after the third day).

II.Discussions
No statistical results can be calculated at all, since the measures of two of the four cases begin only at the 4th day.It is suggestive to notice anyway that in all the cases an excellent regrowth of the original Co-R (in mm) is valuable.The recovery of the viscoelasticity of the dermal component and the hydration of the stratum corneum are well established.
References
[1].Hermanns-Lê T, Hermanns JF, Lesuisse M, Piérard GE: Cyclic Catamenial Dermatoses;Biomed Res Int. 2013; 15(64) 59.[2].Brasad P:Principles and Practice of Medicine a TB for Students and Practitioners.Jaypee Brothers Publishers.1997.Calcutta[3].3)Berk DR, Bayliss SJ. Milia:a review and classification. J Am Acad Dermatol. 2008 Dec. 59(6):1050-63.[4].Sachdeva M, Kaur S, Nagpal M, Dewan SP. Cutaneous lesions in new born. Indian J Dermatol Venereol Leprol. 2002 Nov-Dec. 68(6):334-7.[5].Langley RG, Walsh NM, Ross JB. Multiple eruptive milia: report of a case, review of the literature, and a classification. J Am Acad Dermatol. 1997 Aug. 37(2 Pt 2):353-6.[6].Southwick GJ, Schwartz RA. The basal cell nevus syndrome: disasters occurring among a series of 36 patients. Cancer. 1979 Dec. 44(6):2294-305.[7].Michaelsson G, Olsson E, Westermark P. The Rombo syndrome: a familial disorder with vermiculate atrophoderma, milia, hypotrichosis, trichoepitheliomas, basal cell carcinomas and peripheral vasodilation with cyanosis. Acta Derm Venereol. 1981. 61(6):497-503[8].Rasmussen JE. A syndrome of trichoepitheliomas, milia, and cylindromas. Arch Dermatol. 1975 May. 111(5):610-4.[9].Su WP, Chun SI, Hammond DE, Gordon H. Pachyonychia congenita: a clinical study of 12 cases and review of the literature. Pediatr Dermatol. 1990 Mar. 7(1):33-8.[10].Bergman R, Schein-Goldshmid R, Hochberg Z, Ben-Izhak O, Sprecher E. The alopecias associated with vitamin D-dependent rickets type IIA and with hairless gene mutations: a comparative clinical, histologic, and immunohistochemical study. Arch Dermatol. 2005 Mar. 141(3):343-51.[11].Tsuji T, Kadoya A, Tanaka R, Kono T, Hamada T. Milia induced by corticosteroids. Arch Dermatol. 1986 Feb. 122(2):139-40. .[12].van Steensel MA, Jaspers NG, Steijlen PM: “A case of Rombo syndrome”. Br. J. Dermatol.:2001; 144(6): 1215–8[13].Epstein W, Klingman AM. The pathogenesis of milia and benign tumors of the skin. J Invest Dermatol. 1956Jan. 26(1):1-11.
Il revival di un preparato galenico ancestrale chiamato Ceratum atto a ristabilire la normale viscoelasticità delle malattie cutanee pericolose come la
disidrosi iatrogena e per trattare le cicatrici dopo la rimozione delle trichilemmali
Riassunto:
Scopo della mia ricerca è quello di aprire la strada al recupero
di un preparato galenico molto antico, che è non si presenta oleoso o ceroso, e quindi non
può essere definito come unguento.
Ma il cavallo di Troia è quel dispositivo medico che abbiamo ideato (e il suo modus
operandi è abbastanza difficile e ingegnoso) e che è in grado di ristabilire una
viscoelasticità ottimale nella componente dermica della pelle umana e a livello del moisture cutaneo al livello dello strato corneo nei casi patologici che sono rari. e comunemente
impossibili da trattare, come la disidrosi iatrogena e lo stato suppurativo
della pelle quando le minuscole cisti epidermiche eruttive vengono rimosse fisicamente dalla pelle per
ottenere una restitutio ad integrum perfetta e assolutamente priva di anomalie.
Parole chiave: cerato, disidrosi iatrogena, milia eruttiva, sindrome di Rombo,
balistometro.
Ceratum è un termine antico per indicare una sorta di unguento in grado di
aderire fortemente all’epidermide e creare un film viscoso ma resistente sullo
strato corneo lentamente e progressivamente, permettendo a tutti gli ingredienti
che vengono inseriti nella formula di penetrare in profondità e regolarmente
attraverso la pelle in modo assoluto.
Ad esempio una vecchia monografia U.S.P. fa riferimento al Ceratum Juniperi Virginiani e al
Ceratum Resinosus, supplemento di una farmacopea britannica di Samuel Frederick
Gray, 1821, registra il Ceratum citrinum e il Ceratum cerae et resinae flavae,
nella Pharmacopoeia Collegii Regalis Medicorum Londinensis (1824), il Ceratum
Sabinae , il Ceratum saponis, il Ceratum resinae (yclept Yellow Basilicon), il
Ceratum Plumbi compositum, il Ceratum Plumbi acetati, il Ceratum calaminae
yclept Epulotic Cerate e il Cerato della mosca spagnola. così come altri cerati che
devono essere registrati negli Annali della Storia della Farmacia.
Tutti i cerati sono stati preparati sciogliendo la cera gialla e mescolando
lentamente a freddo olio di oliva e tutti gli altri ingredienti per ottenere il
Ceratum appropriato.
Ho creato un cerato moderno, basato sullo stesso metodo di lavorazione
ancestrale, utilizzando la cera bianca, perché presenta un punto di fusione più
basso e cera di jojoba, oltre a squalano, ceramidi e burro di karité.
La novità di questo cerato rivisitato è l’olio di Jojoba, che è considerato
ingrediente principale e non emolliente:l’olio di jojoba contiene il 76% di
acido 11-eicosanoico, un acido grasso monoinsaturo (20 C) che è responsabile
della creazione della barriera flessibile ma resistente sullo strato corneo, in modo che
il vapore acqueo non possa disperdersi assolutamente.
In questo modo, anche se il paziente spalma il Ceratum in una giornata fredda e
secca, tutta l’umidità all’interno del suo derma rimane al livello
intracellulare, e se lo sparge durante una giornata umida e calda, lo strato
lipofilo impedisce la fuoriuscita di tutti gli elementi idrosolubili dall’interno.
Ceratum è dedicato soprattutto a tutti i tipi di disidrosi cutanea iatrogena ed
è suggerito dopo la rimozione delle microcisti eruttive soprattutto nell’infanzia,
per evitare che diventino cisti e / o rimangano come cicatrici permanenti sul
viso per tutta la vita.
La disidrosi cutanea iatrogena è spesso evocata da terapie a lungo termine che
vengono utilizzate per combattere diversi malesseri o da metodi fisici per
diagnosticare altre malattie o curare o dopo interventi chirurgici, e così, ad
esempio, tra le disidrosi causate dall’uso prolungato e dall’abuso di farmaci,
Varietà di farmaci contro la carenza di folato, talassemia, iperglicemia,
sindrome di Nelson / secrezione di ACTH, (1) lichen planus, dermatite
erpetiforme, eritema multiforme, pompholyx, disidrosi progesterone autoimmune,
xerosys indotta di pemfigo / penicillamina, sindrome da dumping, (2)
follicolite, fibrosite e infine abuso di antidepressivi; tra i metodi fisici di
diagnosi delle Radiazioni / ionizzanti / raggi X e tra gli interventi post
chirurgici la surrenectomia bilaterale e talvolta dopo alcuni tipi di situazioni
traumatiche.
Le microcisti, d’altra parte, sono cisti cheratinose benigne che si manifestano
comunemente come minuscole protuberanze bianche sul viso del neonato. Quando
sono presenti sul margine gengivale, sono indicati come macchie di Bohn. Le micromilie
possono essere ampiamente classificate in tipi primari e secondari. Le milie
congenite nei neonati rappresentano la stragrande maggioranza delle milie
primarie. La milia primaria può anche verificarsi in associazione con una delle
numerose genodermatosi o sporadicamente senza risultati associati. La milia
secondaria può essere associata a una malattia della pelle sottostante, farmaci
o traumi.
Berk e Bayliss hanno pubblicato una classificazione aggiornata di milia, come
segue (3)
La milia primaria può essere:
Milia primaria congenita e benigna di bambini e adulti, Milia en plaque, Milia
nodulare raggruppata, Milia eruttiva multipla, Nevo depigmentoso con milia,
genodermatosi.
Le milia secondarie sono spesso associate ad abuso di farmaci o condizioni post-
traumatiche.
Anche le milie acquisite benigne di bambini e adulti si verificano
spontaneamente; tuttavia, come altri milia acquisiti, hanno la tendenza a
persistere senza trattamento. Le milie acquisite benigne di bambini e adulti
colpiscono preferibilmente le palpebre, le guance, la fronte e i genitali.
La milia eruttiva multipla descrive la milia acquisita e diffusa che appare
piuttosto bruscamente nel corso di settimane o mesi. Le milie eruttive multiple
possono essere associate a una genodermatosi o ereditate in modo autosomico
dominante senza altre anomalie apparenti; tuttavia, nella maggior parte dei casi
si verificano sporadicamente.
Milia associata a genodermatosi sono state riportate in associazione con
sindrome del nevo basocellulare, (4) sindrome di Rombo, (5) sindrome di Brooke-
Spiegler, (6) pachionichia congenita tipo 2, (7) e atrichia con lesioni
papulari. (8)
Nei bambini, la milia traumatica si manifesta più comunemente a seguito di
abrasioni o ustioni. Sono state segnalate anche milia a seguito di innesto
cutaneo. La milia può manifestarsi in associazione a vesciche della pelle.
Epidermolisi bollosa e porfiria cutanea tarda sono gli esempi classici. La milia
associata all’uso di corticosteroidi topici è raramente riportata. (9)
Il tipo più comune di rimozione della milia viene eseguito utilizzando un ago.
Una volta pulita la pelle dalla milia, viene quindi utilizzato un ago sterile per
creare una minuscola incisione nella pelle che copre la cisti e il contenuto
della milia viene accuratamente estratto in modo da non causare alcun trauma alla
pelle.
Alcuni tipi di milia potrebbero non essere adatti a questo tipo di rimozione e
potrebbe essere necessario trattare con un laser a impulsi elettrici. Questo tipo di laser è utile per
cauterizzare la pelle che ricopre i milia utilizzando minuscoli impulsi
elettrici quindi consentendo l’estrazione del contenuto.
In altri casi può essere più opportuno prescrivere un farmaco topico per
trattare la milia, ma questo è solo per alcuni tipi di milia, specialmente
quelle eruttive e le milie raggruppate nodulari. (10-11)
Il trattamento migliore dipenderà dal tipo di milia, nonché dalla posizione e
dal numero di milia che devono essere rimosse. Le estetiste suggeriscono
trattamenti utilizzando regolarmente un detergente esfoliante non abrasivo e un
prodotto a base di vitamina A. Le milia tendono generalmente a ripresentarsi,
dopo una leggera microabrasione. Questi prodotti tendono ad ammorbidire la pelle che
copre la milia, rendendola più facile da rimuovere e possono anche aiutare a
prevenire un ulteriore sviluppo di milia.
Dopo la rimozione della milia, i tre strati superiori dell’epidermide vengono
lesi, ed è da esorcizzare il rischio di una cicatrizzazione fuorviante (quasi
alla primissima fase, quella infiammatoria, quando i tessuti possono subire
aggressioni batteriche).
Per questo ho creato un Ceratum, atto a creare una sorta di film ceroso spesso,
che per la sua lipofilia tende a soffocare tutti i batteri Gram positivi e Gram
negativi.
II.Materiali e metodi
Abbiamo reclutato 4 (quattro) volontari che hanno deciso volontariamente di
sottoporsi alle nostre sperimentazioni per nove (9) giorni e abbiamo utilizzato
un ballistometro (ballistometro torsionale Dia-Strom) per valutare l’aumento
dell’idratazione e del grado di viscoelasticità del loro pelle e derma.
Gli individui erano:
1) una donna di mezza età affetta dalla sindrome di Saurat-Kaya. Le
manifestazioni cliniche della sindrome che è concepita anche come dermatoporosi
comprendono marcatori morfologici di fragilità – piuttosto banali – come porpora
senile, pseudoscara stellata e atrofia cutanea ed espressione funzionale di
fragilità cutanea derivante da traumi minori quali lacerazioni cutanee
frequenti, guarigione ritardata delle ferite, ulcere atrofiche non cicatrizzanti
e sanguinamento sottocutaneo con formazione di ematomi dissecanti che portano ad
ampie zone di necrosi. Non riesce mai a stare ai raggi del sole, nemmeno in
inverno e deve usare sempre emulsioni total block screen, e la manifestazione
più importante della sindrome è sotto i suoi occhi e sugli zigomi.
2) una donna anziana (75 anni) che presenta labbra così secche e screpolate che
nessun rossetto o gloss può aderire alla mucosa buccale.
3) un bambino con milia sotto occhi e palpebre (le misure con ballistometro sono
state effettuate solo dopo il terzo giorno di applicazione di Ceratum)
4) una donna di mezza età affetta dalla sindrome di Rombo, una malattia genetica
molto rara caratterizzata principalmente da atrofodermia vermiculata del viso,
milie multiple, teleangectasie, eritema acrale, vasodilatazione periferica con
cianosi (12) e propensione a sviluppare carcinomi a cellule basali (13) ) Le
lesioni diventano visibili nella tarda infanzia, sono iniziate all’età di 7-10
anni e sono più pronunciate sul viso, specialmente sulle le guance. In età adulta, si sono
sviluppate papule giallo-biancastre simili a milia e vasi teleangectasici. Le
papule erano presenti in particolare sulle guance e sulla fronte, diventando
gradualmente molto evidenti e dominando il quadro clinico. In un caso sono stati
trovati tricoepiteliomi. Negli adulti, le ciglia e le sopracciglia erano
mancanti o distribuite in modo irregolare con crescita difettosa e mal
direzionata. I carcinomi a cellule basali erano una complicanza frequente.
L’atrofia cutanea è stata indicata come atrofoderma vermiculata. I carcinomi
basocellulari possono svilupparsi intorno ai 35 anni. Le osservazioni
istologiche durante la fase iniziale includono follicoli piliferi distribuiti
irregolarmente e atrofici, milia, vasi dermici dilatati, mancanza di elastina o
elastina in grumi. Come nel caso precedente le misure con il ballistometro sono
state eseguite solo dopo il terzo giorno di applicazione del Ceratum.
Il Ballistometro è uno strumento progettato per valutare in vivo, in modo non
invasivo, le proprietà viscoelastiche della pelle analizzando il modello di
rimbalzo di una sonda simile a un pendolo quando impatta sulla pelle. L’energia
cinetica della sonda che colpisce la pelle viene immagazzinata dai componenti
elastici della pelle e viene quindi rilasciata, provocando il rimbalzo della
sonda. Poiché la pelle è un materiale viscoelastico e anisotropo, l’altezza del
rimbalzo della sonda è influenzata dalla quantità di energia immagazzinata persa
nella viscosità della pelle. In questo modo il Ballistometro misura la capacità
della pelle di assorbire energia meccanica e valuta principalmente il
comportamento dei tessuti sottostanti lo strato corneo.
I risultati sono rappresentati graficamente da una curva dove più fattori sono
responsabili dei valori finali (registrati come coefficiente di restituzione)
che vanno da 0 a 1 mm.
I suddetti fattori corrispondono
α) Rientro: la profondità di penetrazione del picco della punta della sonda
sotto il livello della pelle (datum della pelle)
K: l’altezza iniziale della punta della sonda sopra la superficie della pelle.
Questo è direttamente correlato all&) #39;energia immagazzinata nel filo di torsione
b
γAlpha: il tasso di smorzamento dell’energia. Valori grandi indicano
campioni assorbenti di energia (inelastici)
δ)) Coefficiente di restituzione – CoR: un valore alto indica a
campione altamente elastico
Area: l&ε)) #39;area tra il profilo di rimbalzo e la pelle
zero dato
La curva è rappresentata come segue, dove è possibile osservare che i valori
reali vanno da 0 e 1mm.
Immagine 1
Questi valori sono derivati dalle altezze del primo e del secondo rimbalzo,
misurate come l’ampiezza dello spostamento angolare della sonda. Le
Le altezze del
primo e del secondo rimbalzo sono direttamente correlate all’elasticità della
pelle, in quanto un materiale più elastico produce un rimbalzo maggiore quando
viene colpito dalla sonda rispetto a un materiale meno elastico, assumendo una
viscosità equivalente (Fthenakis, et al.1991). Sebbene queste variabili siano
comunemente considerate indicatori della natura elastica della pelle, l’ampiezza
e / o il numero di spostamenti della sonda possono trasmettere altre qualità,
come la compattezza o la morbidezza della pelle (Jemec et al. 2001). Il
coefficiente di restituzione si riferisce alla proporzione dell’altezza massima
che la sonda rimbalza dopo aver colpito la pelle. Il coefficiente di
restituzione può variare da 0, se l’impatto era completamente privo di
elasticità, a 1, che è uno stato teorico di elasticità completa (Fthenakis, et
al. 1991).
III.Discussioni
Non è possibile calcolare alcun risultato statistico, poiché le misure di due
dei quattro casi iniziano solo al 4 ° giorno.
È suggestivo notare comunque che in tutti i casi è pregevole un’ottima
ricrescita del Co-R originale (in mm).
Il recupero della viscoelasticità della componente dermica e l’idratazione dello strato corneo sono così eccezionalmente assicurati.